Forensics of Femoral Nail Failure
Fractographic Analysis of Femoral Nail Failure
MD-Lab supported a clinical forensic engineering investigation into the mechanical failure of a proximal femoral nail assembly. The project focused on fractographic analysis of the recovered hip screw and sleeve, translating fracture-surface evidence into a clear explanation of how the implant failed.
Impact
The work connected clinical evidence with mechanical failure analysis. After the implant failed and was removed during revision surgery, the central question was not only that the fixation had failed, but why the hip screw and sleeve had fractured in that pattern.
MD-Lab’s fractographic assessment gave the medical team and implant stakeholders an engineering basis for interpreting the failure. By examining the recovered components and the fracture surface morphology, the analysis supported an abrupt brittle fracture caused by combined bending and torsional loading, with no relevant signs of progressive fatigue on the examined surface.
MD-Lab’s Contribution
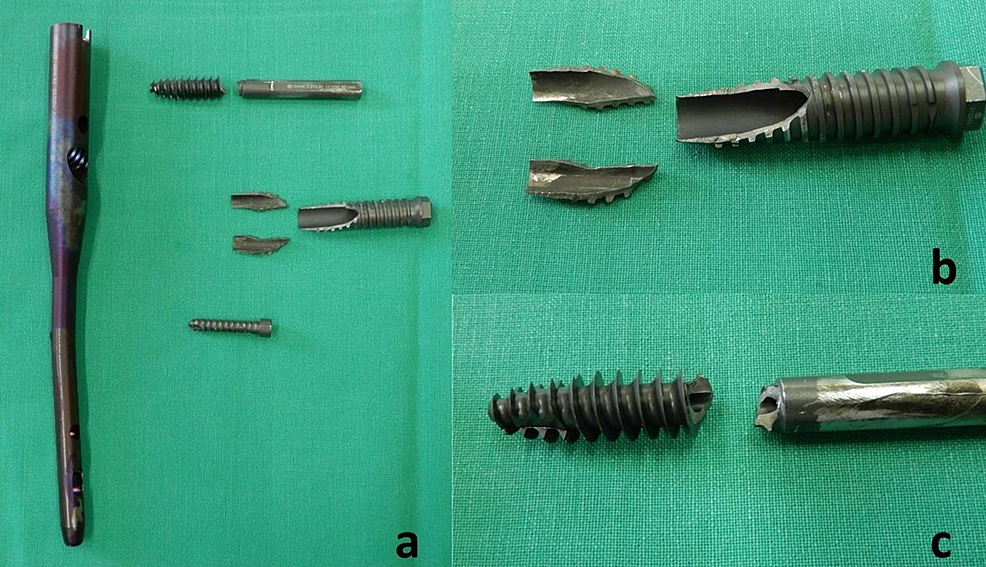
MD-Lab received the broken implant after revision surgery and focused on the mechanical reading of the failure surfaces. The team first assessed the recovered debris macroscopically, noting rough fracture faces with uniform texture, close surface matching and no evident necking that would indicate plastic deformation before failure.
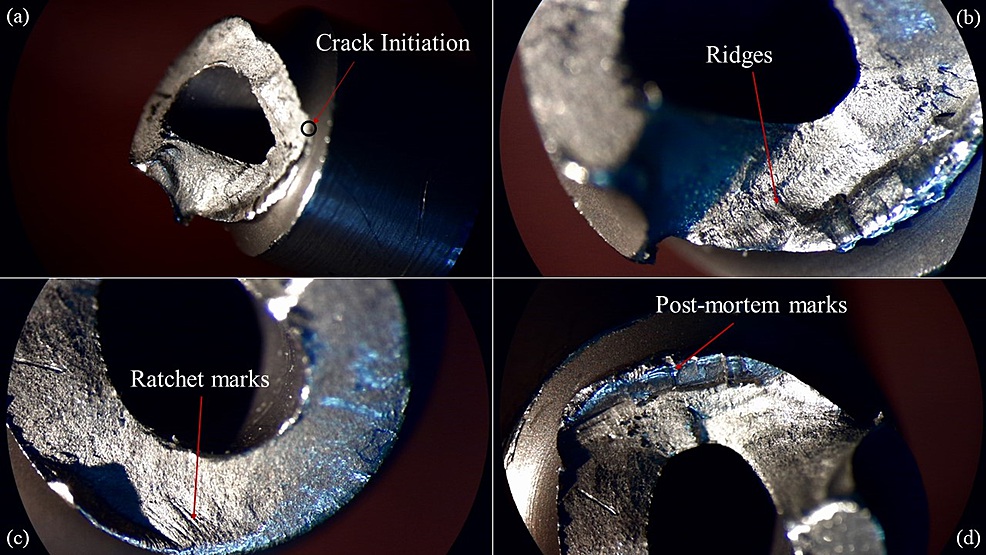
The fracture surface of the broken hip screw was then examined using stereoscope imaging. This allowed the team to locate the crack initiation area near the start of the thread, identify the inclined crack propagation path, and evaluate features such as ridges, ratchet marks, roughness and the absence of beach marks.
Scope of the Work
The project addressed a demanding clinical and engineering question: whether the implant failed through gradual fatigue, a material or manufacturing issue, implantation-related damage, or a sudden overload event. That distinction matters because each explanation leads to different lessons for implant design, surgical decision-making and patient management.
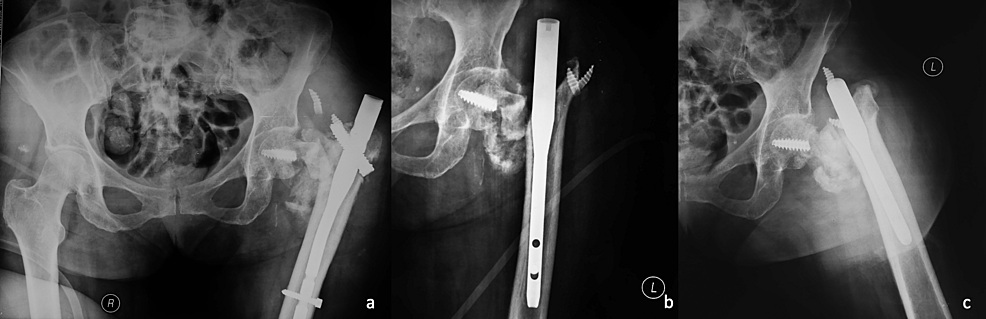
The project scope therefore combined the case record, radiographic evidence, retrieved implant fragments and laboratory fracture-surface interpretation. MD-Lab’s role was the engineering core of that scope: turning the physical evidence from the failed metal components into a defensible failure mechanism.
Why Fractography Was Needed
The same clinical endpoint, a broken implant, can result from very different mechanical histories. A fatigue failure would suggest stable crack growth under repeated loading, while overload failure points toward a sudden event or loading state that exceeded the local capacity of the screw assembly.
Fractography was needed because the recovered metal surface retained this history. The analysis looked for markers such as crack origin, propagation direction, roughness, ratchet marks, ridges, beach marks, corrosion, oxidation, calcification and plastic deformation. The absence or presence of these features allowed the team to move beyond visual damage description and toward failure-cause interpretation.
- The crack initiated near a thread transition where stress concentration was expected.
- The crack propagated at approximately 50-55 degrees to the screw axis before following the thread helix.
- No beach marks were identified on the examined surface, weakening the fatigue-failure explanation.
- The rough, closely matching fracture faces supported sudden brittle fracture due to overloading.
Contribution to the Project
The fractographic findings helped close the loop between the clinical case and the mechanical explanation. Instead of leaving the failure as an unexplained implant breakage, MD-Lab’s analysis supported a specific mechanism: abrupt brittle fracture under combined bending and torsion, with fatigue and chemical attack not supported by the observed fracture-surface evidence.
This contribution made the case useful beyond a single patient record. The engineering interpretation provided evidence that surgeons, researchers and manufacturers can use when evaluating implant behavior, reviewing fixation strategies and improving future orthopedic hardware under demanding loading conditions.





